


Dan Culhane, 62, took extraordinary precautions when he returned to the ice as a youth hockey referee in January. He triple-masked, wore a plexiglass face shield on his helmet and donned his gear at home to minimize time indoors.
It wasn’t enough.
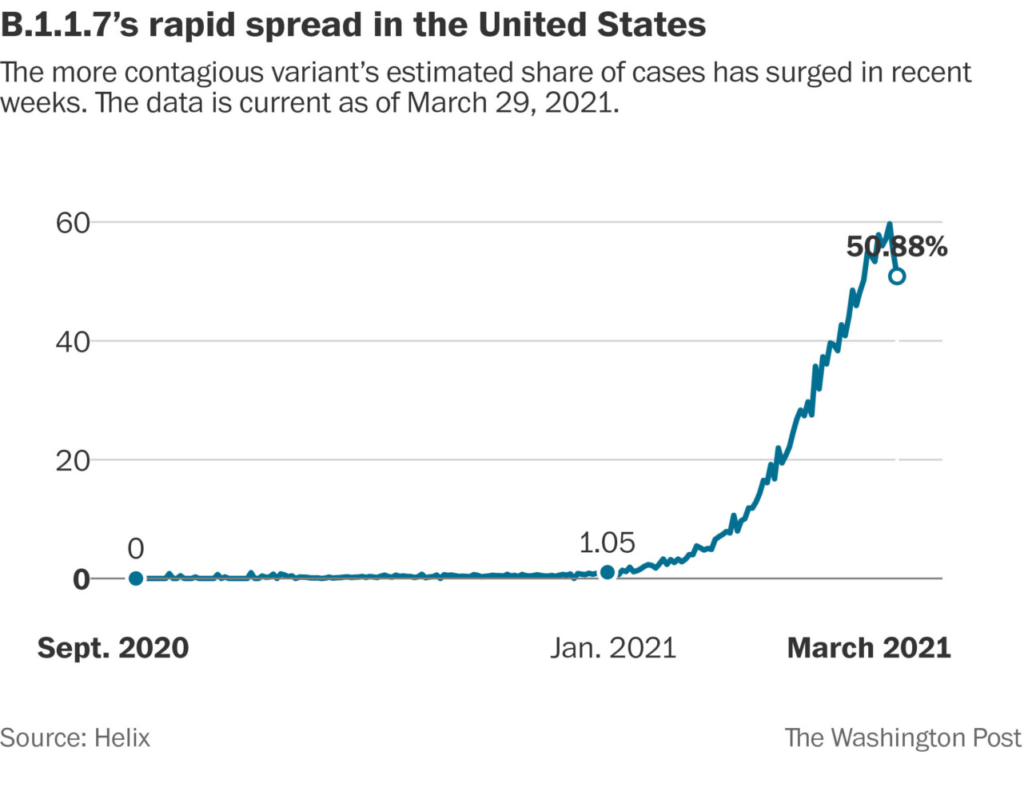
Culhane, who died on Feb. 28 of COVID-19, is one of more than 189 people confirmed or suspected to be linked to an unusual youth sports outbreak of the coronavirus in Carver County, Minn., driven by the B.1.1.7 variant that was first seen in the United Kingdom. The interlinked cases span all levels of K-12 schools, from elementary to high school, and 18 hockey, four basketball, three lacrosse and one soccer teams.
“Until now we haven’t seen transmission like this in kids in the pandemic,” said Michael Osterholm, an infectious-disease specialist at the University of Minnesota who served as an adviser to President Joe Biden.
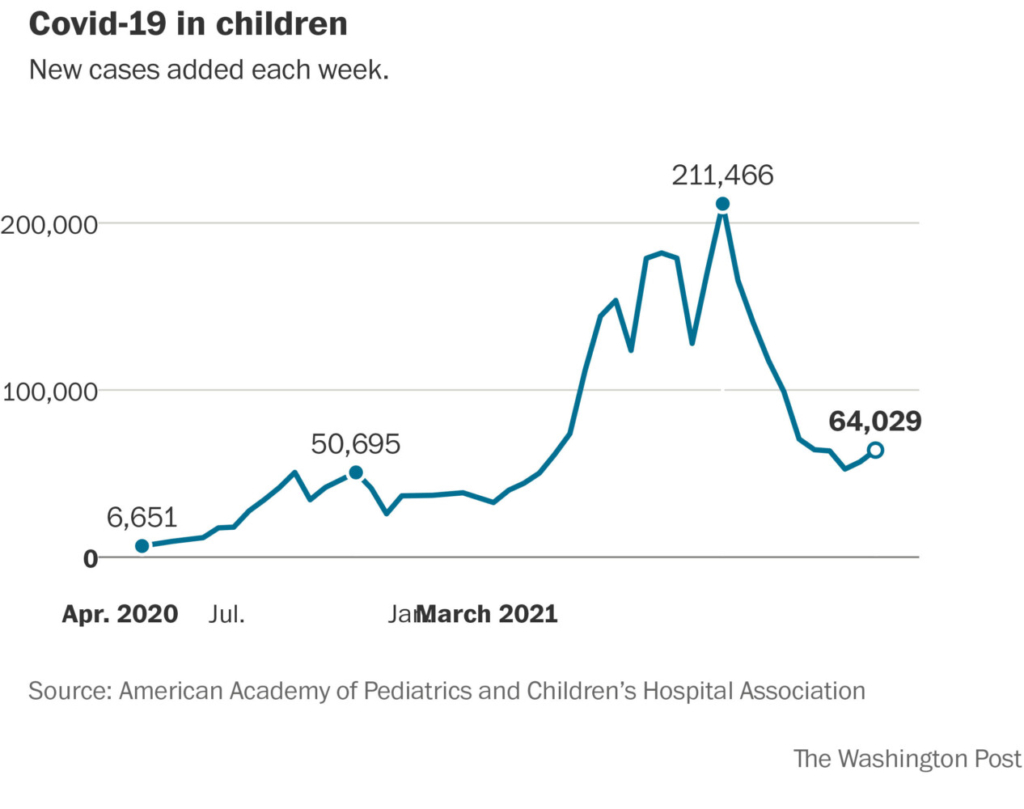
After a surge of infections among children peaked in January, a new wave has been building since mid-March, and many worry about the risks to vulnerable, still-unvaccinated adults such as Culhane. Even as coronavirus cases in the United States remain far off their peaks as vaccinations accelerate, 63,862 new COVID-19 cases among children, representing 18 percent of the total, were reported for week ended April 1, according to data collected by the American Academy of Pediatrics and the Children’s Hospital Association. A growing number of them are caused by virus variants, which represent a big unknown in what is otherwise a time of national optimism: The question is whether these emerging B.1.1.7 clusters foreshadow the surges seen in parts of Europe, where they upended school openings and a return to normalcy, or are just a blip on the way to the end of the pandemic in the United States, given the pace of vaccinations here.
Minnesota’s case numbers, which had been falling since December, recently began inching upward again.
In Nevada, the B.1.1.7 variant – which has been confirmed in several studies to be more infectious – has been linked to an outbreak at a recent youth volleyball tournament. In Michigan, cases among those ages 10 to 19 have jumped 133 percent during the past month, faster than any other age group, and the state’s leading epidemiologist said the infections seem to have been spread through activities “including sports, but not limited to sports,” rather than in the classroom.
Many of these outbreaks involving young people “are related to youth sports and extracurricular activities,” said Rochelle Walensky, director of the Centers for Disease Control and Prevention, at a briefing Monday. She noted that CDC guidance calls for limiting those activities and urged Americans to “please continue to hang in there and continue to do the things that we know prevent the spread.”
Officials say they believe transmission may be happening through athletic activities, rather than in the classroom, because some sports such as wrestling, basketball and volleyball involve close indoor contact. They have also wondered whether outbreaks may be triggered by related interactions such as carpooling, sleepovers and team celebrations, when people let their guard down, rather than from the practices and games themselves.
The rise in infections in children has so far not resulted in a surge in pediatric hospitalizations. As in the past, most cases in children have been mild, health officials say, but they worry about vulnerable adults interacting with them, such as coaches, instructors, child-care providers or parents. Across the United States, a number of youth sports coaches have become seriously ill or died during the past few months as activities have opened up.
In December, COVID-19 took the life of Jamie Seitz, 51, an assistant basketball coach in Denver, N.C., whose team made it to the state championships last month. In January, it also killed Chris Beerman, 53, director of Lexington United Volleyball, a club for girls ages 9 to 18. On March 29, it killed Damien Jackson, a high school math teacher in Columbia, S.C., who coached the girls’ track and field squad and served as the offensive coordinator for the football team. Genomic sequencing has directly linked some adult cases to youth outbreaks, but the technology isn’t widely available, so others have been associated through contact tracing.
The changing demographics of COVID-19, the disease caused by the novel coronavirus, are prompting a radical shift in testing strategies to prioritize asymptomatic children and teens. Numerous jurisdictions are moving testing sites to sportsplexes, recreation centers or other locations convenient to where games and practices are held.
On April 2, youths ages 13 to 19 in Michigan began tobe tested before all practices and competitions, per an order from Gov. Gretchen Whitmer, D. Suffolk County, a suburb of New York City, became the first in the state to require weekly testing for kids participating in high-risk sports, such as high school wrestling and basketball. Numerous counties in California are doing the same.
Minnesota recommends that all school-age kids returning to school and their families get tested every two weeks, and that student athletes and those involved with other in-person activities get tested weekly.
NEW OUTBREAKS LOOK DIFFERENT
For most of the pandemic, SARS-CoV-2 has spread in big bursts that have been described by epidemiologists as viral bombs. The Biogen conference in Boston, a church in South Korea, a French ski resort. In each of these events, infectious-disease investigators were able to trace the cases back to one highly infectious “patient zero.” This uneven transmission, with an estimated 20 percent of people infecting many others, while 80 percent spread the virus to no one or just a few, has been a hallmark of the virus since the very early days.
The recent outbreak in Carver County looks very different.
Kris Ehresmann, the Minnesota Department of Health’s director of the division of infectious diseases, describes the 189 cases – 49 of which were confirmed to be B.1.1.7 through genomic sequencing and the rest of which are suspected to be the variant – as having more of a “lattice” pattern in which each node is connected to several others. She also said the variant appears to have a high attack rate in households between children and parents and siblings. In a report, her team commented that the youth clusters have seeded community spread “to a degree not seen in previous spikes.”
“It isn’t just the sheer number of cases, but the network of interconnectivity that is striking,” she said. “It is showing us how readily transmissible this virus variant can be.” She said it’s as if the virus has mapped the area’s whole social ecosystem.
Felix Wong, a Massachusetts Institute of Technology postdoctoral fellow who has been modeling coronavirus transmission throughout the pandemic, found in an analysis for The Washington Post that a measure of the “clustering” aspect of the Carver County spread is different from past outbreaks. Last year, studies show the pandemic was largely driven by a few superspreaders infecting many. But in Carver County, the data suggests the transmission pattern is more similar to the flu, in which a greater number of people spread the virus to a few others.
Wong cautioned that this is just one case study and more data is needed to make stronger conclusions. He said the higher transmission rate of B.1.1.7 should lead to larger and more frequent superspreading events. But changes such as masking practices, vaccinations and natural immunity from previous infections may prevent that. He also noted our ability to contract trace effectively is hampered by the sheer magnitude of the infections.
“Nowadays the case numbers are so high it’s difficult to figure out where the huge clusters are when the virus has more or less spread around everywhere,” he said.
MINNESOTA PLEADS FOR PAUSE
The outbreak in Carver County began in one of the least likely places – a K-8 school. When Minnesota’s genomic sequencing team on Feb. 16 noticed a pair of B.1.1.7 cases there, contact tracing teams sprang into action. They found multiple additional cases among students and staff, sports groups they played for and members of their households. Within a few weeks, cases in the larger community had taken off.
For Osterholm, the outbreak was eerily reminiscent of what happened in November in Kent, an English county at the southeastern extreme of the United Kingdom. The country had been under a national lockdown, but cases were still climbing in that region, overwhelming hospitals. By far the fastest rise was among those ages 11 to 18, prompting officials to mandate testing for all youths to break chains of transmission. It wasn’t until Dec. 10 that British experts identified the new variant and speculated that it had an easier time entering cells.
“That would put children on a more level playing field, if you like,” Wendy Barclay, head of the Department of Infectious Disease at Imperial College London, commented at the time.
“From my perspective, I think we haven’t fully felt the effects of B.1.1.7 and many have been far too quick to dismiss the danger,” Osterholm said. “I think it’s going to be a challenge.”
When the Minnesota Department of Health first confirmed the outbreak, it pleaded with sports organizers and families for a two-week pause on activities.
Few complied.
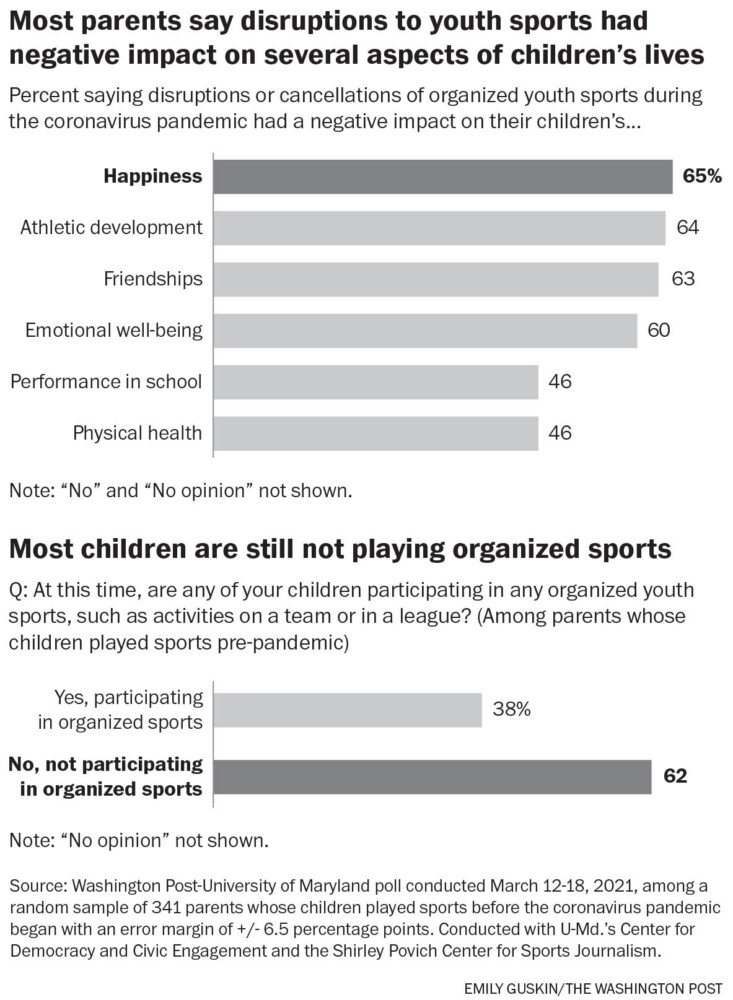
Most parents say disruptions to youth sports had negative impact on several aspects of children’s lives Emily Guskin/The Washington Post
That reaction was not entirely unexpected, as youth sports have become one of the most impassioned reopening debates. In Montgomery County, Md., parents peppered roads with signs that declared, “Youth Hockey is not a community health risk.”
In San Diego, Phoenix, Detroit and many other large cities, parents protested in the streets, insisting sports are essential not only for children’s physical health, but also for their social and mental health.
As the technology and availability of coronavirus testing have improved over the past few months, many jurisdictions have settled on increased testing as an alternative to shutdowns.
The Michigan High School Athletic Association has just wrapped up a pilot program with wrestling teams that allowed students to be tested weekly by their school nurses. Geoff Kimmerly, the group’s communications director, said students who tested positive were immediately sent home to isolate, keeping outbreaks to a minimum. The message is “starting to sink in,” he said, that those who want to participate in sports should follow precautions.
This week, the state is rolling out weekly testing to 100,000 public school athletes who participate in spring sports. “From an administrative view, that’s a lot, so some schools and leagues are frustrated,” Kimmerly said. “But it’s the right thing to do. Our students, schools and families will do whatever is required to continue to play.”
Mark Pandori, the director of the Nevada State Public Health Laboratory at the University of Nevada at Reno, said a recent youth volleyball tournament is generating “a very, very large cluster” of B.1.1.7 cases. He said the lab identified dozens of secondary cases and is finding additional infections among tertiary contacts, or those with even more degrees of separation.
“We are now at the point of community spread,” he said.
That outbreak was discovered by mandatory weekly testing of a university athlete, who attended the volleyball tournament, he said, noting that such monitoring is becoming an important tool given the speed at which some of the variants spread.
In sports-crazy Minnesota, tensions have been high between public officials, schools and families with young athletes. In November, after Gov. Tim Walz ordered youth sports paused to slow the spread of the coronavirus, one group – “Let Them Play MN,” organized via Facebook – sued in U.S. District Court to end the suspension. In January, it protested the state’s mask mandate for high school players, arguing that it could cause breathing issues and reduced vision that could lead to falls and concussions.
David Adney, executive director of the Minnesota Association of Secondary School Principals, said that “to shut down everything doesn’t make sense.” When schools have moved to introduce new restrictions or policies, “you get a lot of pushback from the community,” he said.
In recent weeks, however, some groups have reached a compromise. Minnesota officials set up a drop-in testing site at the Chanhassen Recreation Center in Carver County to make it more convenient for athletes to get tested.
Ehresmann, the state’s infectious-disease expert, said the additional testing has not only helped kids stay in sports, but it has also given epidemiologists a picture of how the new variant is moving in the community. The positivity rate in Carver County the first few days the testing site was operating was 6.9 percent – much higher than 3.9 percent in the rest of the state during the same period.
“We definitely have had good uptake,” she said of the testing site. “There were some sports and some teams that said yes we’ll do a two-week pause, and others that said we’re not going to pause but we will institute regular testing for our participants. And that’s great, too. That gets to the heart of where are cases occurring, and how they keep them from spreading.”
VARIANT SEEMED FAR AWAY
Of the 189 linked cases in Carver County, two people – both adults – were hospitalized. Although health officials did not identify people in the cluster, family members have spoken out about relatives being part of the group.
For Dan Culhane of Minneapolis, it started with a slightly runny nose on Feb. 11 that he thought was probably allergies. The radio production director had recently finished stem cell treatment for multiple myeloma and was thrilled when his doctors cleared him to venture out into the world again with the proper precautions. He and his wife, Nancy, had been very strict about self-quarantining and had not been out even to a grocery store for nearly a year. He immediately signed up to referee youth hockey again, as he had done for the past 20 years.
Nancy was nervous, “but it was just something he had to do,” so she supported him. The B.1.1.7 variant was still something that seemed far away.
Culhane had refereed a couple of games about 40 miles out of town in Carver County shortly before he got sick. His condition deteriorated quickly, until he was hospitalized on Feb. 23.
The next day, Brandt Vettel, a 50-year-old who coaches freshman basketball at Chanhassen High School in Carver County, texted his wife that he was “aching,” but she thought nothing of it, because he also mentioned that he had done sprints and push-ups with the team. By the next morning, however, he had a fever of 101, and the day after that, he tested positive for the coronavirus. He was soon admitted to the hospital on supplemental oxygen.
Vettel’s condition stabilized and he was discharged home. His wife, Kari, a physician assistant who had been fully vaccinated before he became ill, cautioned family and friends. “That is the variant that caused the U.K. to shut back down,” she wrote on Caring Bridge,a health journal site. “I have watched my husband, a fit 50-year-old be so sick.”
But Culhane’s condition nosedived. He was put on a ventilator and then, Nancy recalled, “he went on a downward spiral.” He had a spiking fever. His liver readings were through the roof, and his kidneys had stopped functioning. He was bleeding and clotting at the same time in the brain and died at 5:27 a.m. on Feb. 28.
“In retrospect, I wish he would have never done it,” Nancy said. “I don’t blame the hockey. I don’t blame anybody for that. It was something he loved. He took all the precautions. And it’s such an insidious virus that I don’t know how it could have been prevented.”
The Washington Post’s Alice Crites contributed to this report.
Send questions/comments to the editors.
