



Sgt. Adam Howard, left, and Sgt. Kevin Sager of the South Portland Police Department demonstrate on Saturday how a drug recognition expert measures pupil size and reaction. Sager is one of the 110 police officers in Maine who is a drug recognition expert. Police and prosecutors believe drug recognition work will grow in the state following the legalization of recreational marijuana. Michele McDonald/Staff Photographer Buy this Photo
Richard Tanguay is not a drinker or a drug user.
So, the 69-year-old career school bus driver said it was a frightening surprise when on a November evening, as he ferried about 30 high school athletes and their coaches back to Biddeford from a championship game, he was pulled over by a state trooper and later accused by police of being under the influence of drugs.
“In a matter of half an hour, 42 years of my life (as a bus driver) went down the toilet,” Tanguay said about the arrest. Police publicized the incident, and Tanguay was condemned by his community. “I was, in a matter of speaking, guilty until proven innocent.”
But police got it wrong.
A urine sample later showed Tanguay was not under the influence of drugs or alcohol, and the Cumberland County District Attorney’s Office let the case go in January with no charge. This month, Tanguay resumed driving a school bus for the Biddeford school department.
Tanguay’s case highlights the sometimes difficult work of accurately determining whether a driver is impaired by drug use given the lack of an instantaneous test such as a Breathalyzer that screens for alcohol use. And the challenge is about to get a lot bigger.
The number of drugged-driving tests are expected to increase in the coming months as the state’s first recreational marijuana shops open to the public. With easier access to pot, police believe, more people will be driving while high, making for more work on the roadway for the 110 police officers in Maine who are trained as drug recognition experts. Marijuana lingers in the system far longer than the immediate effects that cause impairment, so there is no chemical test to prove intoxication.
“When you see the recreational storefronts and it really becomes a tourist-type destination, that’s when we’re going to see it,” said Falmouth police Lt. Jeff Pardue. “My biggest concern is likely going to be with edibles, with people having portion control and new users who are not use to the dosages.”
Police say Tanguay’s case is an aberration, and that taken together, drug recognition experts are largely accurate in making assessments about what types of drugs someone might have taken. By policy, every drug recognition expert, or DRE, keeps a running log of his or her tests, and every year those statistics are sent to the International Association of Chiefs of Police for review and publication.
Critics say the foundation of drug recognition expertise is unscientific and studies performed decades ago do not meet the rigors of the modern scientific community, and that the drug recognition process is stacked against drivers.
“Some courts have said, ‘Look, it’s not admissible as scientific; you can’t bring it in with the imprimatur of science,'” said Tanguay’s attorney, Ed Folsom. “There are some limits, but in most cases, (drug expert testimony) just gets thrown in there. Then it’s up to the jury or the judge to make a determination of what weight to give it.”
****
Unlike a roadside sobriety test, in which a police officer is trying to determine whether a driver is impaired, most people who are tested by drug recognition experts have already been arrested on suspicion of driving under the influence. A trained officer is called in because a driver’s level of impairment does not square with a Breathalyzer test result showing little or no alcohol in the system.

Richard Tanguay had maintained his innocence and is shown here after learning he would not be prosecuted because tests confirmed there were no drugs in his system. Photo courtesy of Jeremy Ray
It was how Richard Tanguay’s case played out, according to Folsom.
Tanguay was pulled over for speeding in a construction zone and changing lanes without a signal, police have said. After Tanguay’s arrest based on a field sobriety test, his breath test showed he had no alcohol in his system, Folsom said. But police still believed Tanguay was impaired. Following a drug recognition expert’s evaluation, Tanguay was booked into jail for OUI-drugs, endangering the welfare of a child and driving to endanger.
Tanguay was placed on paid leave from his job as a bus driver. More than two months later, after results of his urine tests were negative for drugs, his case was quietly dropped.
Police have declined to say what drug or combination of drugs the DRE believed Tanguay had taken, and the Maine State Police denied a Freedom of Access Act request for all documents associated with the arrest, citing Tanguay’s right to privacy. In an interview last week, Tanguay also declined to say what drug or drugs police suspected of being in his system.
While field sobriety tests performed roadside can be a relatively quick process, a drug recognition test is far more extensive. It can take more than an hour, involves 12 steps and at times resemble a yearly physical.
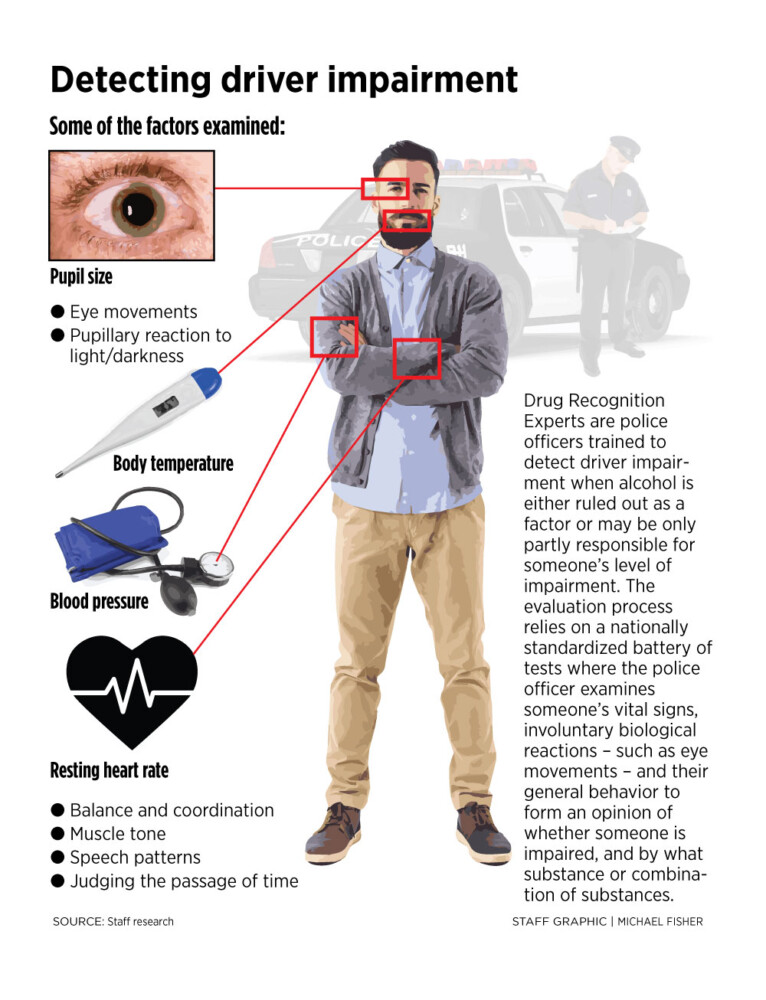
Police ask about medical conditions, prescribed medication, how much sleep someone has had recently and what they ate or drank. They measure and record pulse rate, blood pressure, body temperature and pupil size and pupil reaction to changes in light conditions.
They feel a person’s muscles to see if they are overly tense or abnormally limp. They look up nostrils and examine tongue coloration, even noting the scent of someone’s breath. All of the measurements are compared to average values. Every part of a person’s observable behavior can also be a factor in making a determination of impairment. They perform coordination tests, measure involuntary physiological responses, such as eye movement, and test a driver’s ability to multi-task or accurately gauge the passage of time.
Results found outside of a statistical norm can become a piece of the impairment jigsaw puzzle.
When the tests are complete, the drug expert typically tells the person what type of drugs are suspected to be causing impairment. There are seven broad categories: Depressants, stimulants, hallucinogens, dissociative anesthetics, narcotic analgesics, inhalants and cannabis. This can include legally prescribed medications, as well as illicit drugs.
The DRE’s opinion can be as important to a prosecution as the toxicology results. The presence of a drug in someone’s system does not always mean impairment at the time the person is driving, but rather, it’s the opinion of the officer indicating impairment that is supported by the toxicology, according to the statute.
“If a drug recognition expert has probable cause to believe that a person is under the influence of a specific category of drug (or drugs), … that person must submit to a blood or urine test selected by the drug recognition expert to confirm that person’s category of drug use and determine the presence of the drug,” it says.
Drug expert testimony is also deemed categorically admissible in court by a state statute passed in 2011, but it can still be challenged by a defense attorney or come under scrutiny during cross-examination.
And expert predictions do not always have to be 100 percent accurate to be used by a prosecutor. Only when a driver is believed to have taken a single drug and that substance does not show up in the person’s blood or urine is the opinion considered incorrect.
When two types of substances are suspected, only one has to be found in a toxicology test for the prediction to be considered accurate. When an officer identifies three types of substances, two must be present in the chemical test for the evaluation to be considered accurate.
During training, officers spend two weeks in a classroom and then must complete a dozen evaluations in the field under the supervision of a more experienced drug expert. To be certified, police must make accurate predictions in six cases.
Because so few DRE cases occur in Maine each month, it would be impractical for students to wait around here for a dozen opportunities to hone their training. When funding permits, the Maine Criminal Justice Academy flies trainees to larger jurisdictions such as Baltimore’s city jail, or the county lockup in Maricopa County, Arizona.
In two days, 14 recent DRE trainees performed 168 practice evaluations – more than a quarter the number of all tests performed in 2018 in Maine – on real suspects at the Arizona jail, speeding their transition to full-time certified drug experts, said James Lyman, the training coordinator at the criminal justice academy who oversees the DRE program in Maine.
The pure diversity of substances found there is far greater, and there are more suspects who need evaluations, he said. “You’d see PCP or meth out there. We’d probably see two a year in Maine, but they see it all the time.”

South Portland police Sgt. Kevin Sager, one of the 110 police officers in Maine who is a drug recognition expert, at the computer in his police car on Saturday. It’s lit by a red overhead light, a safety precaution so that police officers aren’t as visible when they’re working. Michele McDonald/Staff Photographer Buy this Photo
South Portland police Sgt. Kevin Sager, who’s been a DRE for five years, said that some suspects react with amazement when he informs them of his opinion.
“I say, ‘Hey, here’s what I think; do you want to tell me something you haven’t already told me?'” Sager said. “Sometimes they’ll be like, ‘Oh, wow, how do you know that?’ And then some will say ‘No, I didn’t take it.'”
Factors such as age, weight and medical condition also factor into the process and can complicate an assessment. Sager said that older drivers are held to the same standard of impairment, but he may use different methods to reach his conclusion.
“We may do alternative tests, such as an alphabet test,” Sager said. For instance, he said, “my dad wouldn’t be able to do most of the tests roadside. He’s got type 2 diabetes. He’s a little overweight, so I’ll do alternative tests.”
Folsom, Tanguay’s attorney, said the age issue is an area of potential bias.
“What happens when someone doesn’t perform well because they’re older?” Folsom said. “They’re impaired, according to the DRE, but what are they impaired by? Well, age. Because (the police) are always thinking in terms of impairment.”
****
Lyman, who runs the DRE training programs, said most of Maine’s drug experts are at least 90 percent accurate in their judgement when compared to lab tests. The accuracy standard to be recertified every two years is 75 percent, Lyman said. That means an officer can get one out of four assessments wrong and continue to do the work.
In the past, the accuracy rating was only calculated when a drug expert’s certificate was up for renewal. Lyman said he could not provide information about the number of drug experts whose accuracy rates were close to the cutoff, and no one at the academy currently tracks the statewide accuracy rate for drug recognition experts, although Lyman has the data in hand. The analysis is simply not performed.
“I can go into (records for) Officer X and look at his accuracy and say, ‘Hey you’ve got a 95 percent accuracy rating,'” Lyman said. “I don’t have a process right now to say the average in the state of Maine.”
But last month, the International Association of Chiefs of Police, which oversees the drug recognition program with the endorsement of the National Highway Transportation Safety Administration, launched a new version of its drug expert tracking database, which will give state managers including Lyman a real-time look at evaluations being performed around the state.
“In the past, I might not know a DRE has a problem with accuracy for two years until that person comes up for recertification,” Lyman said.
In 2018, there were 4,328 cases in which someone’s license was suspended or revoked in Maine because of a charge of driving under the influence. Of those cases, drug recognition experts were involved in about 14 percent, or 620 cases, according to state records.
About 2 percent of DRE evaluations – 13 cases – were like Tanguay’s, where a drug recognition expert formed an opinion that a driver was impaired by drug use, but the toxicology tests showed no drugs or substances, according to the IACP annual report for 2018. That’s slightly better than the national rate of 2.6 percent of 40,749 drug evaluations performed nationally in 2018.
Slightly less reliable, according to the data, are the initial field sobriety tests conducted on the side of the road before a drug recognition expert is called for help.
In 2018, there were 52 cases, or 8.4 percent of all DRE cases, in which someone was arrested for OUI based on a field sobriety test but passed a breath test for alcohol and was then deemed to be unimpaired after the more comprehensive drug evaluation. Nationally, that rate was about 5.8 percent of all DRE cases being cleared without a finding of impairment.
In Maine there were another 22 instances, about 3.5 percent of all DRE cases, in which drivers who were initialed judged to be impaired were in fact experiencing a medical event not related to drugs or alcohol. This is more than twice the national rate, of about 1.4 percent of cases in which a medical issue was mistaken for impairment. It is unknown whether those cases resulted in charges or if they were later dismissed by a district attorney.
Police say that, in cases of medical impairment, they typically inform the Bureau of Motor Vehicles, which has the power to take administrative action against someone’s license if the person is not medically cleared to drive.
****
The business of teaching police officers to recognize drivers impaired by drugs or substances other than alcohol began in the late 1970s, and it did not start with doctors, but with cops.
Traffic officers within the Los Angeles Police Department were frustrated that drivers who seemed clearly to be impaired were passing breath-based alcohol tests.
It proved ineffective and unwieldy to ask doctors and nurses, who are trained in medicine and not specifically to recognize impairment. Impairment fades with time, and without a round-the-clock medical staff, asking for medical tests was pointless, according to a history of the program published by the LAPD.
So the police developed their own standards by “borrowing extensively from medicine, psychiatry, physiology, toxicology,” according to the LAPD’s history. By the early 1980s, the ad hoc practices developed by Los Angeles police were formalized into a curriculum. The National Highway Transportation Safety Administration funded three studies to test the methods, and the results showed that the tests were largely accurate.
By 1988, a standardized curriculum developed by the LAPD and federal highway regulators was adopted by Congress and folded into the omnibus drug bill. DRE training expanded rapidly, driven by federal dollars and a desire to fight the ill effects of illegal drugs on society. A year later, in 1989, the International Association of Chiefs of Police assumed oversight of the training and data collection.
As of 2018, there were 9,116 certified drug recognition experts in the United States – 110 of them in Maine – and more are trained every year.
But the accuracy of those three foundational studies performed the late 1980s and early 1990s has come under attack as unscientific and poorly designed experiments that were biased to help the police, according to Dr. Greg Kane, a physician from Denver who is a professional witness in medical malpractice cases but who has also testified about the unreliable, unscientific nature of field sobriety tests and drug recognition opinions.
Kane evaluated the studies using modern methods designed to ferret out bad experimental methodology that can skew results and published his criticism in 2013 in the Journal of Negative Results in BioMedicine.
In general, Kane found the studies lacked the modern rigor of a truly scientific process. In two of the studies, Kane points out, the only cases evaluated were people who were already judged by one police officer to be impaired. In one of them, test subjects who did not exhibit obvious signs of impairment were excluded.
Different states have also developed a variety of standards for interpreting DRE evidence in court, and so far there is no national case law for attorneys everywhere to follow.
The issue of scientific reliability is currently under consideration by the New Jersey Supreme Court, which agreed to hear a challenge on whether DRE methods are truly scientific and therefore reliable.
And last week, a judge in Rhode Island cleared a man of the most serious charges he faced, after a DRE determined he was under the influence of marijuana at the time he crashed his car, killing a pedestrian. The judge rejected the DRE’s opinion of impairment. The toxicology showed trace amounts indicating consumption long ago.
“We don’t have any way to correlate any amount of a substance in a person’s blood to impairment. … With alcohol we do,” the Rhode Island judge said during the trial, according to the Providence Journal. “This drug area is a complete fog.”
Send questions/comments to the editors.
